We analyzed over >70,000 activities from 305 users that took GLP-1 medication to understand how GLP-1 influences exercise and physiological responses to exercise, more specifically the responses of minimum heart rate and HRV (RMSSD) which we found to be altered by GLP-1 in the previous blog.
Since self-reported data is highly subjective and noisy, we enforced strict cohort selection. Only users with weekly self-reports, or at least a total of 20 entries, and at least 10 days of data prior and posterior medication onset were included. Activity sessions with a maximum heart rate below 120bpm or a duration outside 10 minutes to 3 hour range were excluded to avoid automatic or noisy records.
We used linear mixed and fixed effects regression models to understand the effects of exercise and GLP-1 on heart rate and heart rate variability when accounting for individual user differences, weekday and weekend effects. We ran two different tests, one on total daily exercise time, and the other on exercise time deviation from a 7-day rolling baseline.
HR and HRV
Across both analyses, GLP-1 treatment was associated with significant changes in autonomic physiology. After GLP-1 treatment initiation, minimum heart rate increased by approximately 1.1-1.2 bpm (p ≈ 2.6 × 10⁻⁶). At the same time, nighttime HRV (RMSSD) decreased by roughly 1.7–1.8 ms (p < 10⁻⁴). These results were consistent across both modeling approaches.
These findings suggest that GLP treatment is associated with higher resting cardiovascular activation and reduced parasympathetic activity, indicating increased physiological load reported across studies[1].
GLP-1 responses to absolute exercise load
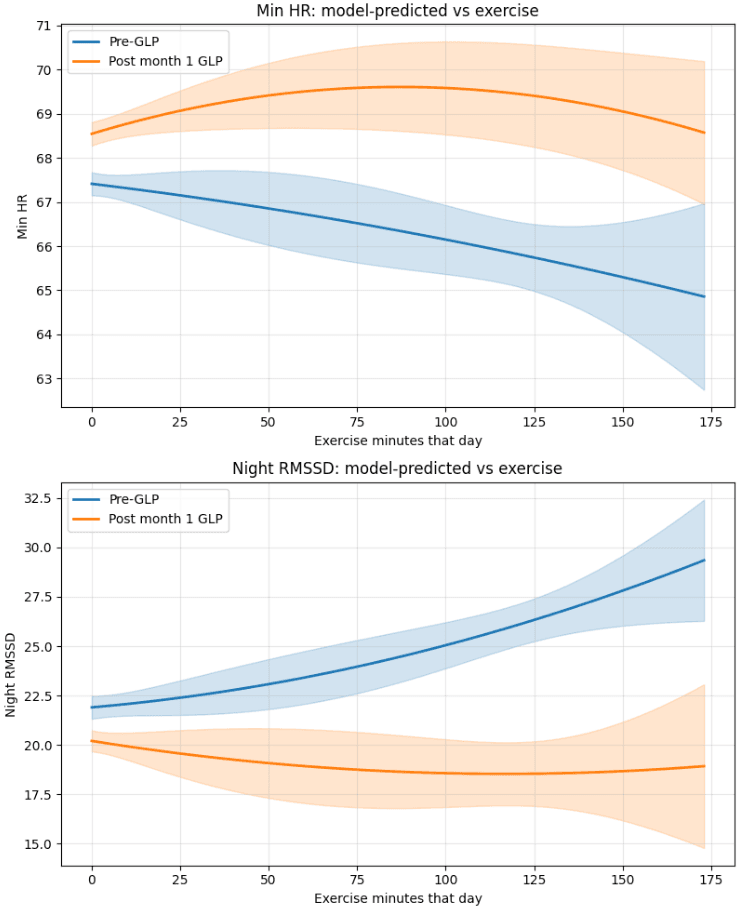
The combined nonlinear interaction between GLP treatment and exercise load was highly significant for both HR and HRV, while exercise alone was not. This indicates that the relationship between exercise and physiological recovery differs before and after GLP treatment.
Before GLP treatment, individuals who exercised more tended to show lower minimum heart rates and higher HRV. This pattern likely reflects differences in baseline fitness: individuals who regularly perform longer workouts are generally more fit and therefore exhibit lower resting heart rate and higher HRV[2].
After GLP treatment initiation, this pattern changes. Minimum heart rate initially increases with exercise duration, before declining slightly at very high exercise levels. This suggests that while GLP increases cardiovascular strain overall, individuals with higher fitness levels may partially mitigate these effects at higher exercise volumes[3].
For HRV, the pattern differs. HRV drops after GLP treatment and remains relatively flat across exercise levels. This indicates that fitness does not appear to offset the HRV-reducing effect of GLP treatment, suggesting that GLP-associated physiological load persists even among individuals who exercise more[4].
GLP-1 responses to increasing exercise load
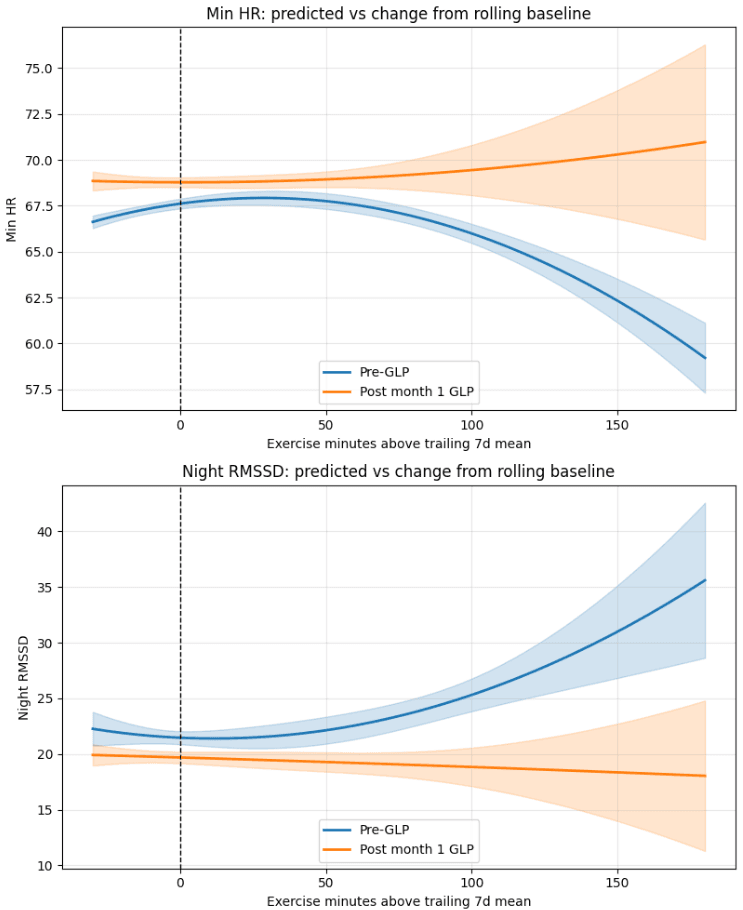
The second analysis examined exercise relative to each individual's recent activity baseline, defined as the difference between that day's exercise duration and the individual's trailing 7-day average. This approach isolates the effect of increasing or decreasing training load relative to one's usual routine, rather than absolute exercise volume.
The second analysis examined exercise relative to each individual's recent activity baseline, defined as the difference between that day's exercise duration and the individual's trailing 7-day average. This approach isolates the effect of increasing or decreasing training load relative to one's usual routine, rather than absolute exercise volume.
Before GLP treatment (blue curve), minimum HR initially increases slightly when exercise exceeds the rolling baseline but then declines substantially at very large deviations. This likely reflects a selection effect, where individuals capable of exercising far above their typical baseline tend to be more physically fit and therefore exhibit lower resting heart rates and higher HRV.
A similar pattern is observed for HRV. Before GLP treatment, HRV increases strongly as exercise exceeds the rolling baseline, again consistent with fitter individuals performing larger training loads. In contrast, after GLP initiation, HRV remains consistently lower and relatively flat across exercise deviations, indicating that GLP treatment reduces HRV regardless of increases in exercise load[3].
Overall, these results suggest that GLP treatment alters the physiological response to exercise load. While individuals appear able to tolerate small increases in exercise relative to their normal routine, larger increases in training load are associated with higher heart rate and persistently lower HRV during GLP treatment[5].
Conclusion
Across both analyses, GLP treatment is associated with higher minimum heart rate and lower nighttime HRV, suggesting increased physiological load and reduced recovery during sleep. These effects are consistent across models and remain significant after controlling for individual differences and weekday effects.
There is also some evidence that baseline fitness may mitigate part of the HR response to GLP. Individuals who tend to exercise more show lower minimum heart rates overall, and at higher exercise volumes the HR increase associated with GLP appears smaller. However, this pattern does not appear to apply to HRV, which remains consistently lower after GLP initiation regardless of exercise levels.
Looking at exercise relative to a person’s usual routine provides additional insight. Large increases in exercise above an individual’s typical weekly level are associated with higher minimum heart rate, suggesting increased physiological strain. In contrast, small increases in activity (roughly up to ~30 minutes above baseline) show little change in recovery metrics. This suggests that overall fitness may help buffer some effects, but sudden increases in training load may still stress recovery, particularly after GLP initiation.
Importantly, these results are observational and should not be interpreted as medical or exercise advice. They simply describe associations between GLP use, exercise patterns, and wearable-derived recovery metrics.
Finally, these findings align with earlier observations from the dataset showing lower daily step counts after GLP initiation. The combination of higher HR, lower HRV, and reduced activity may reflect changes in recovery capacity, which could plausibly contribute to reduced physical activity levels.
References
[1] Liu J, Wang Y, Zhang X, et al. Effect of glucagon-like peptide-1 receptor agonists on heart rate in patients with obesity: a systematic review and network meta-analysis. Front Endocrinol (Lausanne). 2026;17:1291857. doi:10.3389/fendo.2026.1291857.
[2] Gronwald T, de Bem Alves AC, Hoos O, Hottenrott K. What is behind changes in resting heart rate and heart rate variability? A narrative review. Int J Environ Res Public Health. 2021;18(19):10063. doi:10.3390/ijerph181910063.
[3] Grosicki GJ, Kim J, Ogonowski E, et al. Heart and health behavior responses to GLP-1 receptor agonists: a 12-week study using wearable technology and causal inference. Am J Physiol Heart Circ Physiol. 2025;328(3):H450–H461. doi:10.1152/ajpheart.00809.2024.
[4] Jinnouchi H, Yamashita Y, Suehiro S, et al. Effects of Liraglutide on Heart Rate and Heart Rate Variability in Patients With Type 2 Diabetes Mellitus. Diabetes Care. 2017;40(1):117–120. doi:10.2337/dc16-1129.
[5] Hansen KB, Clemmensen C, Seier-Poulsen K, et al. Combined Effects of GLP-1 Receptor Agonist and Exercise Training on Cardiorespiratory Fitness in Patients With Type 2 Diabetes: A Randomized Controlled Trial (NCT04122716). J Clin Endocrinol Metab. 2022;107(5):e1985–e1994. doi:10.1210/clinem/dgab892.