We use cookies to enhance your browsing experience and analyse our traffic. By clicking “Accept All”, you consent to our use of cookies according to our Cookie Policy. You can change your mind any time by visiting out cookie policy.
Melatonin’s Real Effect Peaks on Day 4 - And It's NOT Sleep
Most people take melatonin expecting to fall asleep faster or sleep longer. We analyzed over 200,000 sleep records from hundreds of users and found it does neither. What it does do is lower overnight heart rate and raise HRV, but not until days 3–5 of consistent use. After that, the effect fades. When users stop, there's no withdrawal or rebound. Melatonin works as a timing cue for your body clock, not a sedative.
Melatonin has no measurable effect on sleep duration, latency, or onset — we analyzed 200,000+ sleep records from hundreds of users and found that the thing most people take it for, better sleep, doesn't show up in the data.
It does lower overnight heart rate and raise HRV, peaking around days 3–5 — the effect is statistically significant but fades after roughly a week, suggesting melatonin acts as a circadian timing cue rather than a sedative.
There is no withdrawal or rebound effect — when users stop taking melatonin, metrics return to baseline within two days rather than worsening, with a brief carry-over benefit immediately after stopping.
What is Melatonin? How Does it Work?
Melatonin is a hormone our bodies naturally produce at night, and it acts as a “darkness signal” that helps coordinate circadian timing and nighttime physiology. It targets our brain’s circadian pacemaker (our biological clock) to shift circadian phase. [1]
We analyzed 200,000+ sleep records from hundreds of users who reported taking melatonin at least once. To isolate the effects of melatonin, we excluded the nights where users consumed alcohol, late caffeine or showed illness symptoms (specifically tagged illness). Using linear mixed effect models, we compared nights where users took melatonin vs those where they did not to understand how melatonin influences our physiology and sleep at night.
This is real‑world, self‑reported data with strong within‑person controls, but it is still observational. This blog answers “what changes when we take melatonin compared to when we don’t” but is not equivalent to a clinical trial study. For a comparative analysis across users, we computed the rolling Z-scores for all metrics to let us compare people on different absolute scales (e.g., naturally high or low HRV), but it also means the results are about relative change rather than absolute values.
Just a quick, friendly note: we’re not doctors, and nothing in this post should be taken as medical advice or a recommendation to start (or stop) taking melatonin supplements. We’re simply sharing what the numbers show among people who already track it. And as with anything self-reported, those melatonin tags are only as good as the info people enter, so please keep that in mind.
Get the latest Terra Research reports and insights every week as soon as they're published.
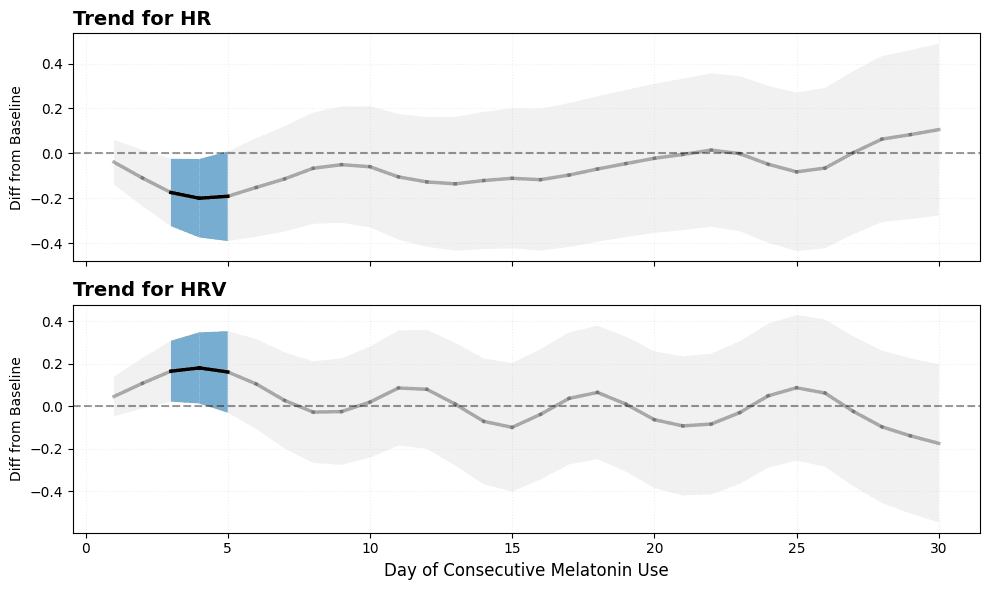
We examined physiological trajectories (breathing rate, average night time heart rate and HRV) over consecutive nights of melatonin use. Each day within a melatonin “burst” was compared against the user’s non‑melatonin baseline using a mixed‑effects model. We focused on bursts up to 30 days to maintain sample size and stability.
Day 1 shows minimal separation from baseline, our body’s physiology looks “the same”. HRV increases and HR decreases over the first few days, with the largest separation around days 3–5. These effects meet our statistical threshold (p < 0.05) and a small‑to‑moderate effect size (|Cohen’s d| > 0.2). After roughly a week, variability across users increases and the average effect attenuates toward baseline.
Breathing rate did not show consistent or statistically significant deviations from baseline.
Figure 1. Trends in overnight heart rate (HR) and HRV (RMSSD) z-scores across consecutive nights of melatonin use. The black line is the LOWESS‑smoothed mixed‑effects estimate; the shaded band shows the 95% confidence interval from the smoothed standard errors. Blue segments indicate intervals where the metrics are statistically different from baseline.
The data shows that the benefit is not immediate for most users; it builds over a few days. After around day 5, the average effect fades and we mostly observe between‑person variation. This suggests melatonin does not have a uniform long‑term effect: some users continue to show improvements while others return to baseline. This pattern aligns with melatonin acting as a timing cue rather than a steadily accumulating sedative effect.
Withdrawal Effects
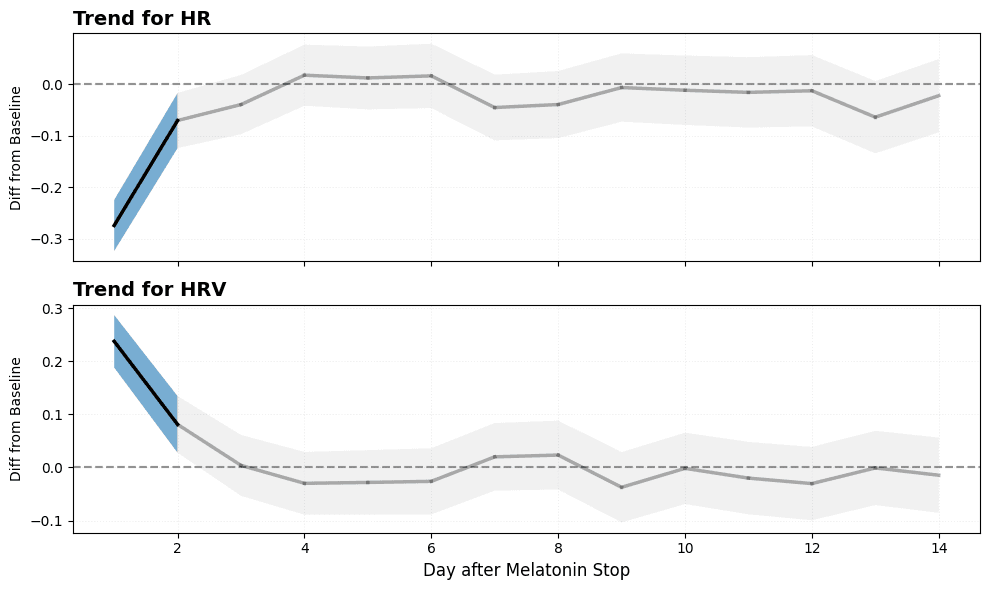
We analyzed the two weeks after a period of consecutive melatonin use and compared those nights to each user’s non‑melatonin baseline using the same mixed‑effects framework.
We observed a brief “carry‑over” pattern: HRV is higher and HR is lower immediately after stopping, but these differences fade rapidly. Within the next 2 days metrics return to baseline level on average.
Figure 2. Trends in overnight heart rate (HR) and HRV (RMSSD) z-scores in the 14 days after stopping melatonin. The black line is the LOWESS‑smoothed mixed‑effects estimate; the shaded band shows the 95% confidence interval. Blue segments indicate intervals where metrics statistically differ from non-melatonin baselines.
What does this mean? If melatonin use is stopped, the body doesn’t appear to experience a withdrawal or rebound effect, and in fact residual benefits are present immediately after stopping.
Physiological Effects on Sleep Performance
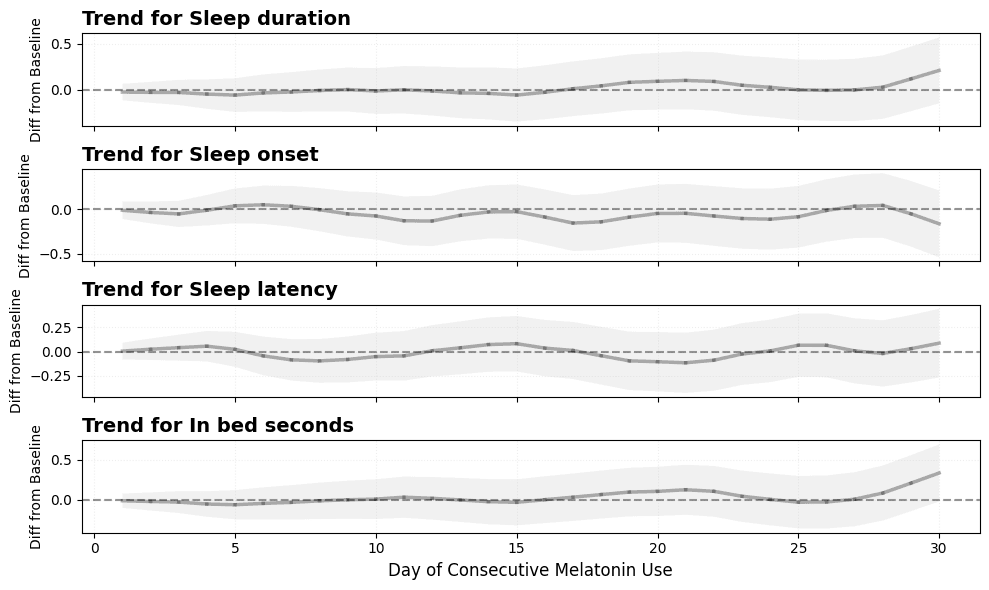
Melatonin has no visible effect on our sleep duration, latency and onset. Counterintuitive?
A possible explanation for this unusual insight is that users might take melatonin on nights they expect to be harder (travel, stress, early wake…) so even if melatonin helps in falling asleep, these tags are reflecting the context rather than the melatonin effects. In fact, clinical studies have also shown modest effects on sleep, which aligns with environmental factors dominating our signal. [2]
Figure 3. Trends in sleep duration, sleep onset, sleep latency, and time in bed z-scores across consecutive nights of melatonin use. The black line is the LOWESS‑smoothed mixed‑effects estimate; the shaded band shows the 95% confidence interval from the smoothed standard errors.
Key Takeaways
Melatonin works best as a timing cue for your body clock, not a sedative that keeps stacking stronger effects night after night [3]. It helps your system recognize “biological night” and can shift circadian timing when taken consistently.
In our data, the clearest benefits weren’t on night one: physiology looked most “recovered” on days 3–5 (lower overnight HR, higher HRV). After roughly a week of continuous use, those HR/HRV differences fade back toward baseline, suggesting melatonin may add less once your rhythm and routine have stabilized. When users stopped, we didn’t see a withdrawal pattern, metrics returned to baseline quickly, consistent with clinical findings that discontinuation of prolonged‑release melatonin is not associated with rebound insomnia or withdrawal symptoms [4].
Finally, melatonin has a greater impact on our physiology than it has on our sleep. Melatonin is often taken on “hard nights,” and clinical evidence suggests its average sleep effects are modest, so real‑world context can dominate these “poor sleep” durations.
References
[1] Liu J, Clough SJ, Hutchinson AJ, Adamah-Biassi EB, Popovska-Gorevski M, Dubocovich ML. MT1 and MT2 Melatonin Receptors: A Therapeutic Perspective. Annu Rev Pharmacol Toxicol. 2016;56:361-83. doi: 10.1146/annurev-pharmtox-010814-124742. Epub 2015 Oct 23. PMID: 26514204; PMCID: PMC5091650.
[2] Asim Alawad, Wala Sati, Sara M I Ahmed, Moayed Elgassim, Mohamad Elgassim, Abderahman Balal, Melatonin-induced symptomatic bradycardia in an otherwise healthy male: a case report, Oxford Medical Case Reports, Volume 2024, Issue 8, August 2024, omae096, https://doi.org/10.1093/omcr/omae096
[3] Liu J, Clough SJ, Hutchinson AJ, Adamah-Biassi EB, Popovska-Gorevski M, Dubocovich ML. MT1 and MT2 Melatonin Receptors: A Therapeutic Perspective. Annu Rev Pharmacol Toxicol. 2016;56:361-83. doi: 10.1146/annurev-pharmtox-010814-124742. Epub 2015 Oct 23. PMID: 26514204; PMCID: PMC5091650.
[4] Lemoine P, Garfinkel D, Laudon M, Nir T, Zisapel N. Prolonged-release melatonin for insomnia - an open-label long-term study of efficacy, safety, and withdrawal. Ther Clin Risk Manag. 2011;7:301-11. doi: 10.2147/TCRM.S23036. Epub 2011 Jul 26. PMID: 21845053; PMCID: PMC3150476.
Summary questions
Does melatonin actually help me fall asleep faster?
In our analysis of 200,000+ sleep records, melatonin showed no visible effect on sleep duration, sleep latency, or sleep onset. This likely reflects the fact that people often take melatonin on already-difficult nights (travel, stress, early wake-ups), so context dominates the signal. Clinical studies similarly find only modest effects on sleep, so don't expect melatonin to work like a sedative.
When does melatonin's effect actually peak?
Not on night one. Across consecutive-use bursts, HRV rose and overnight HR dropped most clearly on days 3–5, meeting statistical significance (p < 0.05) with small-to-moderate effect sizes (|Cohen's d| > 0.2). Day 1 looked essentially identical to baseline — the benefit builds over several nights of consistent use.
Will melatonin keep working if I take it every night?
No — the average effect fades after about a week. Beyond day 7 of continuous use, HR and HRV differences attenuated back toward baseline, with most of the remaining signal coming from between-person variation. This is consistent with melatonin acting as a circadian timing cue rather than a sedative that accumulates stronger effects night after night.
Will I have withdrawal or rebound insomnia if I stop taking melatonin?
The data shows no withdrawal or rebound pattern. In the 14 days after stopping, we actually saw a brief carry-over benefit (higher HRV, lower HR) that faded within about 2 days, after which metrics returned to baseline. This aligns with clinical findings on prolonged-release melatonin showing no rebound insomnia or withdrawal symptoms after discontinuation.
Does melatonin affect my heart rate and HRV more than my sleep?
Yes — that's one of the clearest findings. Melatonin produced statistically significant shifts in overnight HR and HRV around days 3–5, while sleep duration, latency, and onset showed no consistent change. The physiological 'recovery signature' is the real measurable effect; the sleep effect is largely absent in this dataset.
Does melatonin change my breathing rate at night?
No. Unlike heart rate and HRV, breathing rate did not show consistent or statistically significant deviations from baseline across any phase of melatonin use. If you're tracking respiratory metrics expecting a melatonin signal, you likely won't find one.
How was this melatonin analysis actually run?
We analyzed 200,000+ sleep records from hundreds of users who tagged melatonin use, excluding nights with alcohol, late caffeine, or illness symptoms to isolate the effect. Linear mixed-effects models compared melatonin nights to each user's own non-melatonin baseline, with rolling Z-scores so people on different absolute scales (naturally high or low HRV, for example) could be compared. It's observational with strong within-person controls — informative, but not a clinical trial.
Should I take melatonin every night for better recovery?
The data suggests probably not. Benefits peaked on days 3–5 and faded after roughly a week of continuous use, suggesting diminishing returns once your rhythm stabilizes. Melatonin appears most useful as a short-term circadian timing cue — for resetting after travel or schedule shifts — rather than a nightly recovery supplement.