We use cookies to enhance your browsing experience and analyse our traffic. By clicking “Accept All”, you consent to our use of cookies according to our Cookie Policy. You can change your mind any time by visiting out cookie policy.
Sharing a bed adds about 11 minutes of awake time per night. Even comparing the same person on shared vs. alone nights, they still spent around 8 extra minutes awake when a partner was there.
Recovery markers don't agree with each other. Sharing a bed lowers your resting heart rate (a good sign) but also lowers your HRV (a bad sign), and you end up with less time asleep and worse sleep efficiency overall.
People who mostly sleep alone spend the least time awake in bed. Awake time stepped down from 70 minutes (mostly shared) to 66 (mixed) to 57 (mostly alone), while heart rate and HRV differences stayed small and inconclusive.
The conventional wisdom seems to be that having a partner is good for our long-term health. A large part of this benefit should occur when recovery mostly happens, at night. This week’s hypothesis: Sharing a bed makes you sleep and recover better.
I started with a dataset labelled with whether users slept alone or with a partner. This may sound like a bit of fun, and it is, but to the health aficionado looking for every recovery hack, it’s serious business!
I did 4 different types of tests on the data, all in search of an association between bed sharing and improved sleep:
Population-level analysis of shared bed vs alone
Within-person analysis of shared bed vs alone
Users who predominantly share a bed (>75% recorded nights shared) vs users who predominantly sleep alone (>75% recorded nights alone)
A three-way cohort analysis of users who predominantly share a bed (>75% recorded nights shared) vs users who predominantly sleep alone (>75% recorded nights alone) vs the users who sit in the middle (25%→75% shared)
As with all labelled data, we are struggling with the big problem of not knowing whether a user has not labelled something because it doesn’t happen or because they just forgot. At Terra Research, we are working hard on this problem with our Athlete Research club.
The dataset is skewed toward runs of one context (either Bed sharing, or not), with far fewer people who genuinely split their nights in the middle band. We do need to treat the mixed cohort as real, but it is easy to over-interpret.
There are, of course, plenty of reasons to suspect bias in the sample. I imagine it takes a certain person to label data at this level, and maybe the data set is predominantly men or predominantly women. Also, a category of nights could involve plenty of other confounding factors; for example, alone nights may mainly occur when someone is traveling.
Population-Level Analysis
The database contained many more shared-bed nights than alone nights. This is probably what you’d expect with a wearable-wearing sample, but I can’t discount it because users are much more likely to report bed-shared nights than non-bed-shared nights.
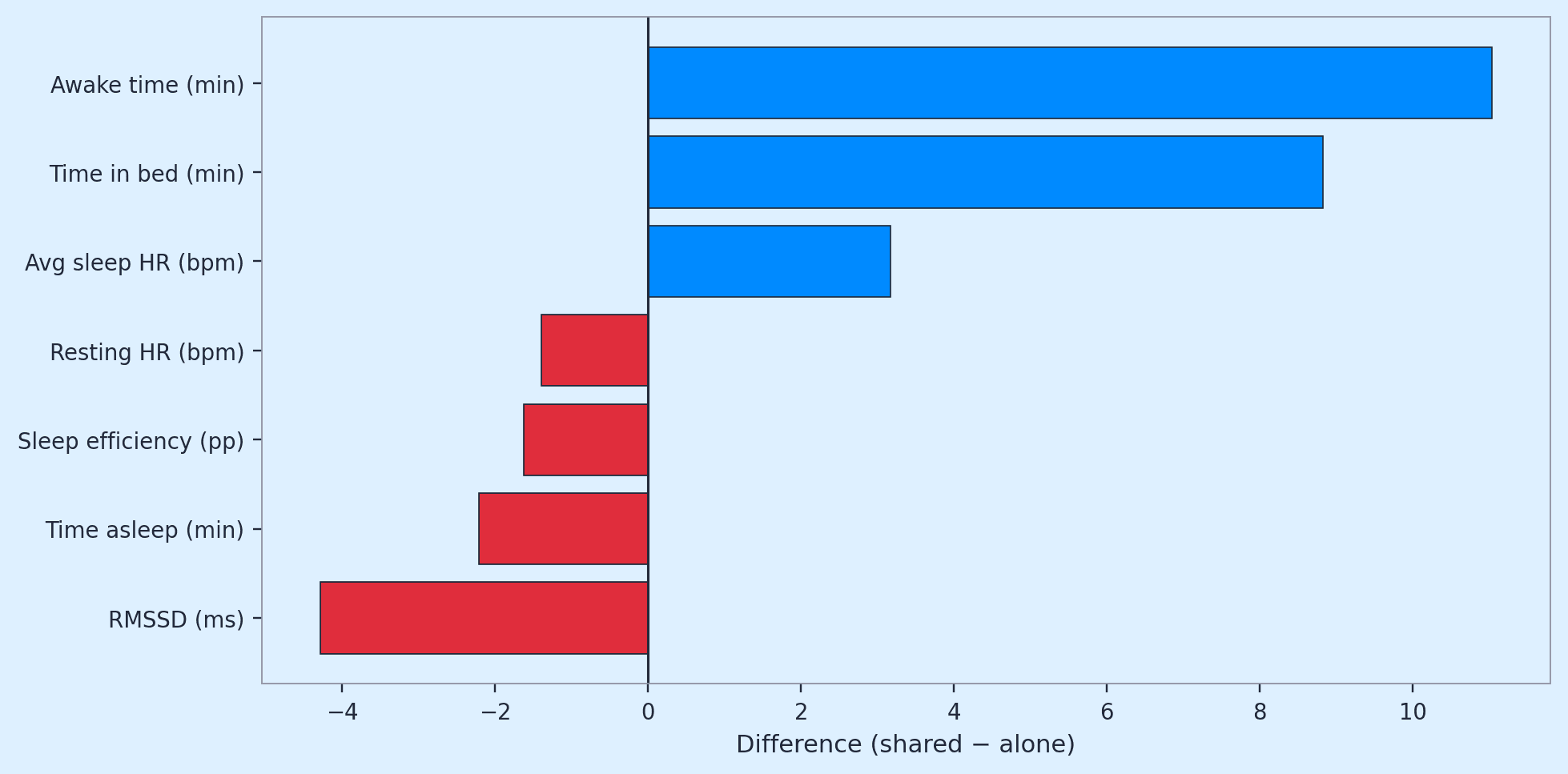
Awake time was about 11 minutes higher on shared-bed nights. Sleep structure was modestly worse on shared-bed nights, as was RMSSD. Most findings were significant, with small effect sizes.
The Heart rate story is where it gets a bit interesting…. Average HR during sleep was higher when sharing, but resting HR was lower on average.
Figure 1: How do standard metrics compare on average between nights where our users shared a bed and slept alone? A hint that bed sharing is better for recovery (Resting HR decreases, but is counteracted by a decrease in RMSSD) even though Sleep efficiency and time asleep decreased?
Get the latest Terra Research reports and insights every week as soon as they're published.
Within-Person (Same User: Shared-Bed vs Alone Nights)
The above cohort analysis compares different people. A stricter question is whether the user, on nights recorded as shared bed, looks different from nights recorded as slept alone. After restricting to people who have both contexts often enough in their history that person-level averages are not pure noise.
I restricted to people with over 3 nights for both labels, and the results were very similar to the population-level analysis. Awake time was the clearest within-person signal, increasing by 8 minutes on shared-bed nights, which is nearly mirrored by a 6-minute decrease in sleep time. In this analysis, I found an increase in resting HR (2.3 bpm, not significant) and a very slight decrease in RMSSD (not significant). These results, along with an investigation of the direction of these relationships for each user in the analysis, show mixed findings, indicating that the data is very noisy.
Dominant context: ≥75% shared vs ≥75% alone (user-level)
Here I am attempting to answer the question: Do people whose history is dominated by one context differ from people dominated by the other?
For each user, I computed the percentage of nights with shared beds and categorized ≥75% shared as “mostly shared,” and ≤25% shared (≥75% alone) as “mostly alone”. I then compared each person’s long-run mean across all their nights (using a Mann–Whitney test on user-level means).
The relationships were the same as in the night-level story: more awake time, slightly less asleep time; lower readiness for shared-dominant; and small HR differences.
One of the big learnings from the previous research and recent literature on sleep is that consistency in health metrics (as measured by the Coefficient of variation, CV) can be more informative than the raw signal. Sleep length CV tended lower (more stable night-to-night) for alone-dominant users when CV was computed with enough nights per person ( ≥50night-per-metric rule for inclusion).
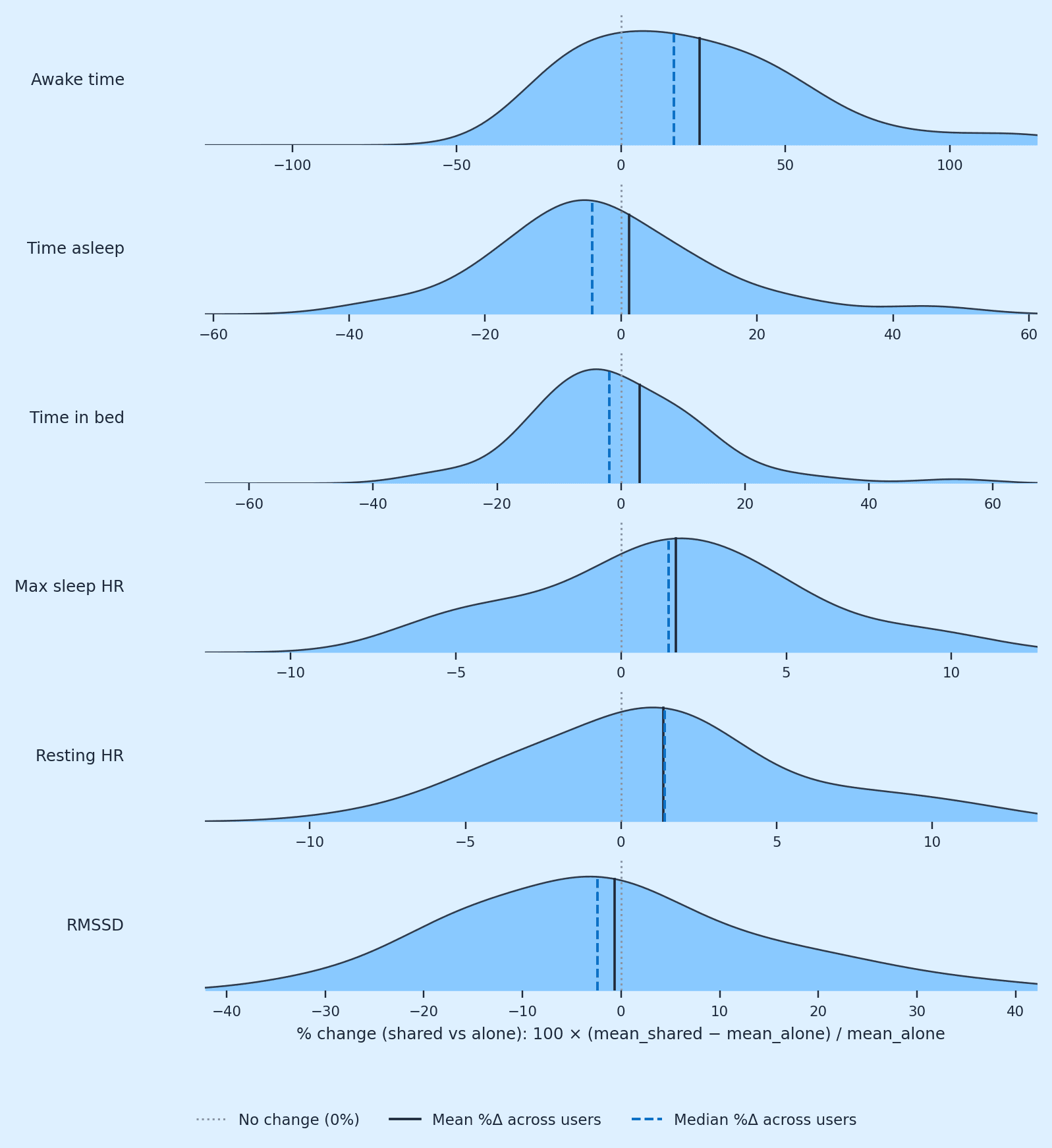
Figure 2: Shows the % change distribution for each variable. The different shapes of the distributions are particularly interesting, as they demonstrate how the mean differences between cohorts are driven.
Three-Way Cohort
Here, I added a third category to the analysis: Mixed (25–75% shared). The signals from the previous analysis all held
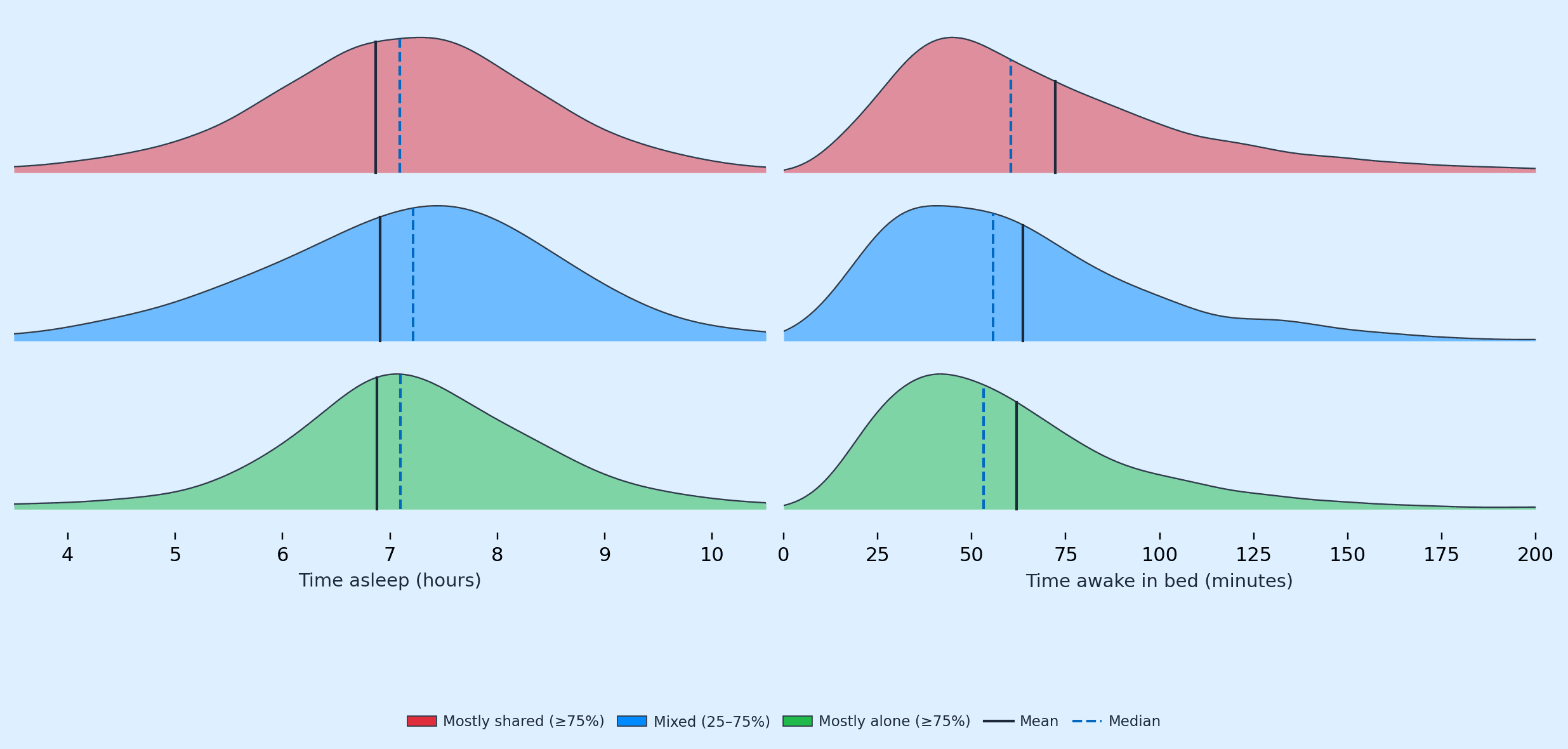
Awake time was highest in mostly shared, middle in mixed, and lowest in mostly alone (70, 66, 57 minutes, respectively). Asleep time was lowest in the mostly shared cohort, middle mixed, and highest in the mostly alone (6.9, 7.0, 7.3 hours). Time in bed: slightly longer, mostly alone (~8.3 h vs ~8.2 h).
Resting HR still sleeps down toward mostly alone with mixed sat in the middle, and max sleep HR is highest when mostly shared.
Figure 3: shows cohort distribution using ridge lines of night-level asleep and awake distributions by group, with mean and median verticals. It demonstrates that the cohort-mean increase in time awake in bed is driven by a long tail, especially in the most-shared cohort.
Checking for Differences
The above analyses show differences between cohorts, but I wanted to know whether these patterns are robust enough to describe. I compared every shared-bed night to every alone night with Welch’s t-test—a two-sample test that asks whether the average on one side differs from the average on the other, without assuming both piles have the same spread. That is a population view: powerful, but it lumps many different people and life situations into two big buckets.
A stricter check looked within the same user: for people who had logged both contexts often enough, I took each person’s typical shared-bed night and typical alone night and computed the difference, then used a Wilcoxon signed-rank test to see whether those person-level gaps cluster around zero.
That test is nonparametric; it works on ranks rather than assuming perfect bell curves, and it is appropriate when you care whether “most people go the same way” rather than whether two perfect normal distributions differ. Here, the signed-rank result for awake time was the stand-out: roughly ten more minutes awake on shared-bed nights for the typical person in that slice, with most individuals pointing in the same direction.
For the two lifestyle cohort analysis, I used the Mann–Whitney U test (another rank-based, nonparametric test). For the three-way lifestyle cohort analysis, I used the Kruskal–Wallis test, the three-group version of the same idea. These tests measure whether at least one group tends to sit higher or lower than the others.
Strong separation for awake and asleep time produced very small p-values and medians that stepped down in order (about 70, 66, 57 minutes awake from mostly-shared to mixed to mostly-alone). RMSSD and heart rate were weak because the three-group tests did not show a reliable shift, HRV medians fell within a similar band, and heart rate differences were small or ambiguous.
What I am trying to test here is whether bed context is associated with systematic differences in sleep structure. Minutes awake (and, more quietly, minutes asleep) are the story, while HRV and HR do not separate cleanly in this dataset. The tests support treating time in bed as the evidence; they do not, by themselves, show that a partner causes the difference, only that, in this observational record, shared-bed context and more fragmented nights tend to travel together.
Time to Head to the Spare Room?
These are associations, not trials. We always have to bear in mind that wearable-derived variables are tracking life in the real world, and all that entails: partners, travel, children, illness, and much more. The mixed cohort is the nearest thing to a crossover group; on timing, it sits between extremes, which I think is a good sign that we are picking up a directionally correct signal.
If you are designing a study rather than reading a blog, the honest next step is to model within-person changes around partner travel, illness, and alcohol, covariates that this dataset may capture, but we don’t know exist!
Thinking of going to sleep in the spare room tonight? I wouldn’t bother unless you’re a hardcore recovery nut, and you’re going to test your own sleep data over 10 plus nights of shared bed and sleeping alone, while controlling as many other factors as you can. If you do collect this data, let me know!
References
Grosicki, G.J., Carter, J.R., Laursen, P.B., Plews, D.J., Altini, M., Galpin, A.J., Fielding, F., von Hippel, W., Chapman, C., Jasinski, S.R., Beattie, U.K. and Holmes, K.E. (2026) ‘Heart rate variability coefficient of variation during sleep as a digital biomarker that reflects behavior and varies by age and sex’, American Journal of Physiology-Heart and Circulatory Physiology, 330(1), pp. H187–H199. https://journals.physiology.org/doi/full/10.1152/ajpheart.00738.2025
Drews, H.J., Wallot, S., Brysch, P., et al. (2020) ‘Bed-Sharing in Couples Is Associated With Increased and Stabilized REM Sleep and Sleep-Stage Synchronization’, Frontiers in Psychiatry, 11, 583. https://pmc.ncbi.nlm.nih.gov/articles/PMC7330166/
Levy Andersen, M., et al. (2025) ‘Interactions between co-sleeping, sleep quality, and relationship health: The benefits and challenges of shared sleep environments’, Journal of Health Psychology. https://journals.sagepub.com/doi/10.1177/13591053251356355
Do I actually sleep better when sharing a bed with a partner?
The wearable data says no — at least not on the metrics that matter most. Across the dataset, shared-bed nights showed about 11 more minutes awake, slightly worse sleep structure, and lower RMSSD compared to alone nights. The conventional wisdom that partners boost recovery isn't supported here on sleep quality measures.
How much more awake time should I expect on shared-bed nights?
Roughly 10 extra minutes awake for the typical person, based on the within-person signed-rank analysis. In the three-way cohort breakdown, mostly-shared sleepers averaged 70 minutes awake, mixed sleepers 66, and mostly-alone sleepers 57 — a clean step-down that's one of the most robust findings in the dataset. Asleep time mirrored this, dropping from 7.3 hours (mostly alone) to 6.9 hours (mostly shared).
Does sharing a bed hurt my heart rate variability?
The signal is weak and inconsistent. Population-level RMSSD was modestly lower on shared-bed nights, but within-person comparisons showed only a very slight, non-significant decrease, and the three-group test didn't show a reliable shift. HRV medians sat in a similar band across cohorts, so HRV doesn't cleanly separate shared vs alone in this data.
Is my resting heart rate affected by whether I share a bed?
The HR story is mixed and counterintuitive. Population-level resting HR was actually lower on shared-bed nights, while average HR during sleep was higher. Within-person, resting HR rose by 2.3 bpm on shared-bed nights but wasn't statistically significant. HR differences across the three cohorts were small or ambiguous — don't read too much into them.
Why am I more restless when sleeping with a partner?
The data can't say causally, but shared-bed context and fragmented nights consistently travel together — the extra ~10 minutes awake shows up at the population level, within-person, and across user-dominant cohorts. Real-world confounders like partner movement, travel, children, and illness aren't controlled for. The signal is directionally consistent, but it's association, not causation.
Does sleeping alone make my sleep more consistent night-to-night?
Yes. Sleep length coefficient of variation (CV) trended lower — meaning more stable night-to-night — for alone-dominant users, when restricted to people with at least 50 nights per metric. Given that recent literature suggests CV can be more informative than raw sleep values, this is a quietly important finding: solo sleepers had more predictable sleep durations.
Can wearable data reliably detect bed-sharing effects on sleep?
For sleep structure, yes — for HRV and HR, less so. Awake time and asleep time produced very small p-values across Welch's t-tests, Wilcoxon signed-rank, Mann-Whitney, and Kruskal-Wallis tests, with medians stepping cleanly across cohorts. HRV and HR didn't separate cleanly. Treat minutes awake as the evidence; treat HR/HRV claims with caution.
Should I move to the spare room to improve my recovery?
Probably not worth it. The effect sizes are small — about 10 minutes of extra awake time and 20-some minutes less sleep at the extreme cohort comparison — and these are observational associations confounded by travel, illness, and life context. If you're a serious recovery optimizer, run your own n=1 experiment over 10+ nights of each condition before committing to separate beds.